via Our Bodies, Our Blog
As part of their ongoing discussion of the about routine mammogram screening for breast cancer, OBOS mentions the complicating issue of breast density.” Dense breasts have less fat and more glandular and connective tissue. While some women’s breasts become less dense and more fatty as they age, other women’s breasts remain relatively dense. Why does this matter? Having dense breast tissue makes it harder to obtain an accurate reading of mammograms. It also increases a woman’s risk of developing breast cancer. However, questions remain about what women should do with that information. In fact, recent research suggests that actual risk of death from breast cancer is not increased for women with denser breast tissue.”
So far, so good. What surprised me is OBOS’ position on “right-to-know” laws that mandate physicians share this information with patients.
“Despite a lack of certainty about how dense breast tissue affects health outcomes, a handful of states have mandated that providers discuss breast density with women. On April 1, California will become the fifth state with a breast density notification law in place. Similar bills have been introduced in other states.
At the federal level, the Breast Density and Mammography Reporting Act was introduced in Congress in 2011, but never made it out of committee. It, too, would require that women be told about breast density, the correlation with cancer, and that they might benefit from supplemental screening tests.”
Since the OBOS’ history is rooted in fighting medical paternalism, I’m puzzled as to why they would oppose efforts to provide women with MORE information. This issue also hits home because I’m “dense” (i.e. have dense breast tissue). Because Connecticut has a right-to-know law and a law mandating health insurance coverage for additional screening, my additional sonograms have not cost me anything but time. Not every woman has these kind of health care benefits, but that’s no excuse for keeping women in the dark about this issue. Sure these added tests are inconvenient and nerve wracking but it’s better than having cancer.
Now, one would think that radiologists would be all over these laws because it means they would get more income, right? Well, it turns out that the American College of Radiology (ACR) opposes right-to-know laws, because, among other things, it would “cause anxiety” in patients and they wouldn’t know how to interpret this data. In a reply to these objections submitted at the National Mammogram Quality Assurance Advisory Board FDA Hearing November 4, 2011, the Institute for Health Quality and Ethics stated:
“There are thousands of medical professionals, researchers, and awareness advocates who have done tremendous work towards advancing the science of breast cancer, from detection to cure. We respect the work that has been done in this field and the many individuals who have dedicated their lives to this commendable pursuit.
However, there is a very real danger here for the ACR and other organizations (equipment manufacturers and prominent breast cancer awareness organizations) which have benefited financially from years of ubiquitous mammogram screening programs. Some of the awareness campaigns and recommendations to women overstate the effectiveness of mammography overall, and completely neglect to inform women of the limited benefits of mammography in dense breast tissue.
Withholding this information from millions of women, many of whom could prevent their premature deaths and years of painful treatment for late stage cancer, calls the motivation of these organizations into question.”
Since I spend a lot of time looking at FDA records for my historical research, I decided to look at the rest of the transcript for this advisory committee meeting. The testimony from breast cancer survivors, including the founders of the patient advocacy organization Are You Dense, reminded me of the women who protested at the 1970 Senate Hearings on the Pill. For example, here’s an excerpt from the testimony of Lynne Farrow from Breast Cancer Choices:
“After the dense breast disclosure was vetoed in California, one of the reasons given was disclosure would cause anxiety in women. I can tell you what causes anxiety in women. Being lied to causes anxiety. Not disclosing that mammography is severely limited in its diagnostic abilities causes anxiety. Not being offered other means of detecting cancer causes anxiety. We are grown women. Our lives are at stake. We don’t want any bureaucrats or insurance companies denying us information because we might get anxiety. We’ll be the judge of what causes anxiety.”
Right on! What’s wrong with a woman’s right-to-know? I’d rather have TMI than not enough.
Update: In reply to a comment I made at OBOS, Rachel writes:
“Thanks for your comments, everyone, and for the added links. Heather, speaking only for myself as an individual – absolutely patient engagement and advocacy is a good thing, but in this case it’s not clear that these laws actually do anything to save women’s lives, and may really just subject them to more and costly tests and interventions. There’s nothing really evidence-based we can tell women to actually do in response to the information. So unless the laws require telling women in the form, “Hey, you have dense breasts, but we don’t really know how to follow up on that, and it probably doesn’t make a difference in terms of your survival,” they’re probably not that helpful. Peggy’s post has a nice exploration of those concerns, by the way. Thanks for commenting.”
Rather than clog up the OBOS comment section, I’ll reply to Peggy’s post here. One of her chief complaints is
the law “violates the free speech of physicians.” She suggests that it might not be a bad idea for radiologists to file a free speech lawsuit. This bothers me since as the
Institute for Health Quality and Ethics report indicated, “free speech” for radiologists includes withholding material medical information from female patients. The report argues “the continued resistance of the ACR and other organizations to providing this material medical information to women has begun to seriously undermine the faith that women have in our medical establishment.” I wrote on Peggy’s blog, “Informed consent is the cornerstone of modern medical practice. It wasn’t that long ago that physicians withheld information from patients (especially women) “for their own good.” Too much information is better than none at all.”
 Recently, the Reproductive Health Technologies Project launched its new Tumblr-based campaign, Healthcare in Our Hands, “The place to celebrate and explore the new status of emergency contraception.” The site invites visitors to submit a photo of themselves with Plan B in their hands (or submit their stories about NOT having trouble getting EC). The RHTP says “your submission will help build RHTP’s map of where Plan B One-Step has been spotted on the shelf nationwide! You can also keep up with the campaign online by following the hashtags #ECOTC and #ECinOurHands on social media.”
Recently, the Reproductive Health Technologies Project launched its new Tumblr-based campaign, Healthcare in Our Hands, “The place to celebrate and explore the new status of emergency contraception.” The site invites visitors to submit a photo of themselves with Plan B in their hands (or submit their stories about NOT having trouble getting EC). The RHTP says “your submission will help build RHTP’s map of where Plan B One-Step has been spotted on the shelf nationwide! You can also keep up with the campaign online by following the hashtags #ECOTC and #ECinOurHands on social media.” this context. In her book, Into Our Own Hands, Sandra Morgen explores how the women’s health movement “shifted power and responsibility from the medical establishment into women’s own hands as health care consumers, providers, and advocates.” Frequently, feminist health activists and drug makers were adversaries — e.g. Barbara Seaman‘s classic expose, The Doctors’ Case Against the Pill, and the
this context. In her book, Into Our Own Hands, Sandra Morgen explores how the women’s health movement “shifted power and responsibility from the medical establishment into women’s own hands as health care consumers, providers, and advocates.” Frequently, feminist health activists and drug makers were adversaries — e.g. Barbara Seaman‘s classic expose, The Doctors’ Case Against the Pill, and the 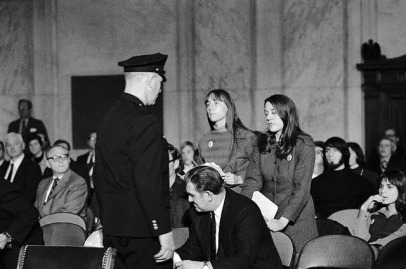 demonstrations by members of DC Liberation (left) at the congressional hearings on the Pill in 1970.
demonstrations by members of DC Liberation (left) at the congressional hearings on the Pill in 1970.